




If you recently came across a headline saying “PCOS has been renamed PMOS” and felt a wave of confusion or even quiet panic you are not alone. Thousands of women who have lived with a PCOS diagnosis for years are asking the same questions: Does this change my diagnosis? Is my treatment still valid? Should I be more worried now?
The short answer is: no, you should not be worried. The science has not changed. Your body has not changed. What has changed is something far more fundamental the medical community has finally corrected a name that was always somewhat misleading. This is a long-overdue update, and it may actually work in your favour.
This historic update, published in The Lancet, aims to more accurately represent the complex and whole-body impact of the condition, which is estimated to affect more than 170 million women worldwide.
Read article : Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process
Let’s walk through everything, calmly and clearly.
What is PMOS?
PMOS stands for Polyendocrine Metabolic Ovarian Syndrome.
This is the new internationally proposed name for what was previously called Polycystic Ovarian Syndrome, or PCOS. The name change has been discussed and supported by leading endocrinologists, reproductive medicine specialists, and women’s health researchers globally.
Breaking the new name down:
- Poly – meaning “many” or “multiple”
- Endocrine – relating to hormones and the glands that produce them
- Metabolic – relating to the body’s energy and chemical processes
- Ovarian – involving the ovaries
- Syndrome – a collection of symptoms that occur together
In simple terms, PMOS is a hormonal and metabolic condition affecting the ovaries and multiple systems throughout the body. This name is more accurate, more inclusive, and more respectful of what the condition actually is which is far more than a problem with cysts. In most women, the ovaries contain multiple immature follicles rather than true cysts. This misunderstanding often delayed proper hormonal and fertility evaluation.
Why PCOS changed to PMOS?
The Old Name Created Confusion from Day One
The term “Polycystic Ovarian Syndrome” has always had a fundamental problem: not every woman with PCOS has cysts on her ovaries. And many women without PCOS do have small follicles that appear cyst-like on ultrasound, which is perfectly normal.
When a doctor told a patient she had “polycystic ovaries,” the immediate mental image of ovaries covered in painful cysts was almost always wrong. These are not cysts in the traditional sense. They are immature follicles that did not ovulate. The name caused unnecessary alarm, misdiagnosis fears, and in some cases, delayed the right diagnosis because a woman did not have visible follicles on her scan.
What the Medical Community Finally Acknowledged
After decades of advocacy from women’s health specialists, patient groups, and researchers, the scientific consensus began to shift. The key recognition was this:
PCOS is primarily a hormonal and metabolic disorder, not simply an ovarian one.
The condition involves:
- Excess androgen (male hormones) production
- Insulin resistance and metabolic dysfunction
- Irregular ovulation and menstrual cycles
- Systemic inflammation
- Psychological and emotional impacts
None of these are captured by the word “polycystic.” The new name – PMOS, Polyendocrine Metabolic Ovarian Syndrome reflects the full picture.
PMOS vs PCOS: What Actually Changed and What didn’t
This is the section most women need to read carefully. Let’s be direct.
What Changed
- The name used in medical literature and, increasingly, in clinical settings
- The framing – PMOS positions this as a metabolic and endocrine condition, not just an ovarian one
- The emphasis – future diagnostic criteria and research will likely expand to address metabolic health more centrally
- The language – removing “polycystic” reduces the stigma and confusion around the word “cysts”
What Did NOT Change
- Your diagnosis – if you were diagnosed with PCOS, you have the same condition now called PMOS
- Your treatment plan – lifestyle changes, medication, supplements, and fertility treatments remain the same
- Your health risks – understanding them and managing them is unchanged
- Your fertility journey – PMOS, like PCOS, is manageable, and pregnancy is absolutely achievable
- Your doctors’ approach – clinicians are not starting from scratch; the medical knowledge base remains intact
The renaming is a refinement. It is not a rediscovery. Think of it as updating the label on a bottle whose contents you already knew well.
Our fertility experts explain that in most PMOS cases, the primary concern is irregular ovulation rather than permanent infertility. With timely diagnosis and personalized treatment plans such as ovulation induction, IUI, or IVF, many women achieve successful pregnancies.
Also read: PCOD vs PCOS: How Are They Different
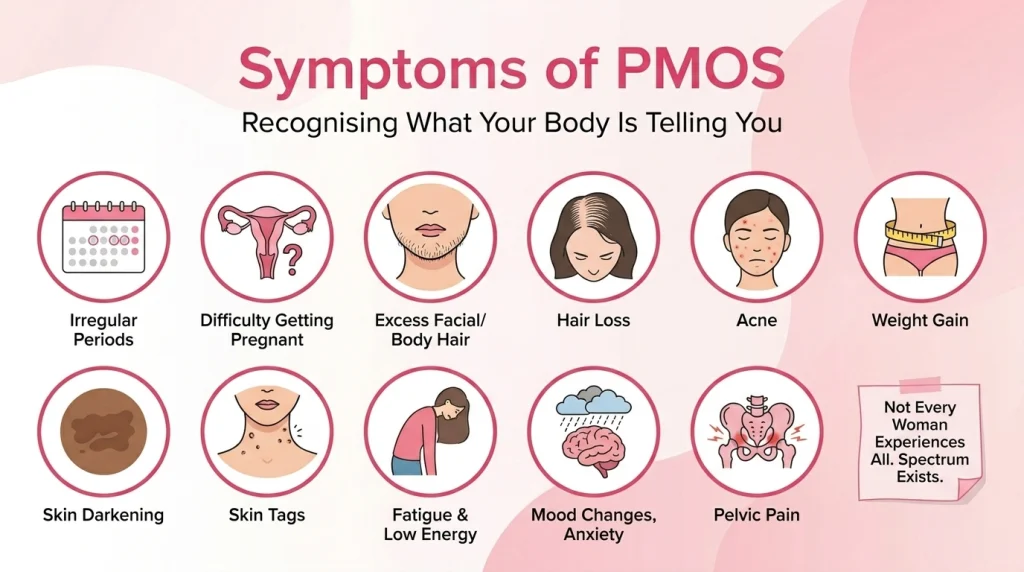
Symptoms of PMOS
The symptoms of PMOS are identical to those previously associated with PCOS. If you were already aware of them, nothing here will surprise you. If you are reading this as someone newly diagnosed or still investigating your symptoms, here is what to watch for.
Common PMOS symptoms include:
- Irregular, infrequent, or absent menstrual periods
- Difficulty getting pregnant due to irregular or absent ovulation
- Excess facial or body hair (hirsutism), particularly on the chin, upper lip, or chest
- Scalp hair thinning or hair loss, especially at the crown
- Acne, particularly along the jawline and chin
- Unexplained weight gain, especially around the abdomen
- Skin darkening in body folds (acanthosis nigricans) — a sign of insulin resistance
- Skin tags
- Fatigue and low energy, especially after meals
- Mood changes, anxiety, and depressive symptoms
- Pelvic pain in some women
Not every woman with PMOS experiences all of these. The syndrome exists on a spectrum, and its presentation varies significantly from person to person. Some women have mild symptoms; others experience significant disruption to daily life. Both are valid, and both deserve proper care.
How PMOS Affects Hormones and Metabolism
This is where the new name truly earns its meaning.
Hormonal Problems
In PMOS, the hypothalamic-pituitary-ovarian axis, the communication system between your brain and ovaries, does not function in the typical way. The pituitary gland often releases luteinising hormone (LH) in excess relative to follicle-stimulating hormone (FSH). This imbalance sends a signal to the ovaries to produce more androgens (such as testosterone and DHEA-S) than is ideal.
High androgen levels are responsible for many of the most visible symptoms: the acne, the unwanted hair, the scalp thinning. They also interfere with normal follicle development, which is why ovulation becomes irregular or absent.
Metabolic Dysfunction
Insulin resistance is present in approximately 70–80% of women with PMOS, even those who are lean and not overweight. When cells do not respond properly to insulin, the pancreas compensates by producing more of it. High insulin levels further stimulate the ovaries to produce androgens, creating a self-reinforcing cycle.
This metabolic dysfunction means that women with PMOS carry a higher long-term risk of:
- Type-2 diabetes
- Cardiovascular disease
- Non-alcoholic fatty liver disease
- Metabolic syndrome
These risks are manageable and that management begins with an accurate diagnosis and a proactive treatment plan. The name PMOS makes it harder for anyone, doctors included, to treat this as “just a period problem.”
PMOS and Fertility: What Women Trying to Conceive Need to Know
This is, understandably, one of the most emotionally charged aspects of a PMOS diagnosis. Many women hear “hormonal disorder” and immediately fear the worst. Let’s address this directly.
PMOS is one of the most common and most treatable causes of female infertility.
The primary fertility challenge in PMOS is anovulation: the ovaries are not releasing eggs consistently. No egg released means no possibility of fertilisation. But this does not mean pregnancy is impossible. It means ovulation needs support.
Also read: Fertility Challenges In PCOS: Strategies For Management And Treatment
Fertility Treatments That Remain Effective for PMOS
- Lifestyle modification – even modest weight loss (5–10% of body weight in women with higher BMI) can restore ovulation in many cases
- Letrozole – currently the first-line oral medication for ovulation induction in PMOS, highly effective
- Clomiphene citrate – another oral ovulation stimulant, used for decades with strong evidence
- Metformin – improves insulin sensitivity, often used alongside ovulation induction
- Gonadotropin injections – for cases where oral medications are insufficient
- IVF (In Vitro Fertilisation) – highly effective for PMOS, with careful monitoring to prevent ovarian hyperstimulation
Women with PMOS who receive proper care have excellent pregnancy outcomes. The fertility journey may require more steps, but the destination is absolutely within reach for the vast majority.
PMOS and Mental Health
One of the most significant shifts the PMOS rename signals is a broader recognition that this condition affects mental health in ways that have long been underacknowledged.
Women with PMOS report higher rates of:
- Anxiety disorders
- Clinical depression
- Body image concerns and disordered eating
- Low self-esteem linked to visible symptoms like acne and hair changes
- Grief and distress related to fertility challenges
These are not secondary concerns. They are central to the experience of living with PMOS, and they deserve the same medical attention as hormonal levels and metabolic markers.
If you are struggling emotionally alongside your physical symptoms, please bring this up with your Fertility Specialist. Psychological support, whether through therapy, medication, or peer support groups is a legitimate and important part of PMOS care.
Does PMOS Treatment Change?
Practically speaking, the transition from PCOS to PMOS in clinical terminology does not require you to change your current treatment. The therapeutic approach remains grounded in the same evidence base.
The cornerstones of PMOS treatment remain:
- Diet – a low-glycaemic, anti-inflammatory diet that helps regulate insulin and androgens
- Exercise – regular physical activity improves insulin sensitivity significantly
- Metformin – for insulin resistance
- Hormonal contraception – for women not trying to conceive, to regulate cycles and manage androgen symptoms
- Anti-androgens – such as spironolactone, for hair and skin concerns
- Ovulation induction agents – for those trying to conceive
- Mental health support – an increasingly prioritised component
What will likely evolve over the coming years, as PMOS gains wider acceptance, is a stronger emphasis on metabolic screening and cardiovascular risk management, earlier, more consistently, and as a standard part of care rather than an afterthought.
What Women with PMOS Should Do Right Now
If this information above has made you feel uncertain about what your next step should be, then here is a practical guide for your help.
1. Do not change or stop any current treatment. Your diagnosis and care plan are valid. Consult your doctor before making any adjustments.
2. Ask your doctor about PMOS. If they are not familiar with the terminology yet, share what you have learned. Not all clinical settings have adopted the new name simultaneously.
3. Request a comprehensive metabolic workup if you have not had one. This includes fasting glucose, insulin levels, HbA1c, lipid profile, thyroid function, and a full hormonal panel. PMOS is a systemic condition and deserves systemic investigation.
4. If you are trying to conceive, consult a fertility specialist. Early intervention dramatically improves outcomes. Do not wait years before seeking help.
5. Prioritise your mental health alongside your physical health. They are not separate concerns in PMOS.
6. Track your symptoms. A symptom journal (periods, energy levels, skin changes, mood, weight). It gives your doctor enormously useful information.
Expert Guidance: What a Fertility Specialist wants you to Know
At Ferty9 Fertility Center, we see women with PMOS (earlier PCOS) every single day. What we consistently observe is that: the women who do best are not the ones who waited and worried. They are the women who came in, asked questions, got answers, and started building a plan. PMOS is not a sentence. It is not a wall between you and the life you want. It is a condition that, when identified and managed, allows women to lead full, healthy, fertile lives.
The name has changed. The hope has not.
Myth-Busting: Common Fears About PMOS
Myth: “PMOS is worse than PCOS. The new name sounds more serious.”
Fact: This is the same condition. The new name is more medically accurate, not more alarming. A more precise label means better targeted treatment.
Myth: “If I have PMOS, I can never get pregnant naturally.”
Fact: Many women with PMOS conceive naturally, especially with lifestyle support. Even those who need medical assistance have high success rates.
Myth: “PMOS means I definitely have cysts on my ovaries.”
Fact: Actually, the whole point of the rename is to move away from this misunderstanding. You may or may not have follicles visible on ultrasound. The diagnosis is based on a combination of hormonal, metabolic, and clinical factors.
Myth: “My PCOS medication won’t work anymore since the name changed.”
Fact: The medication works exactly as it did before. Nothing about pharmacological treatment has changed.
Myth: “I should have been diagnosed with PMOS all along.”
Fact: Your PCOS diagnosis was correct for its time and context. Medicine evolves its terminology as understanding deepens. This is science working as it should.
Must read: Debunking Common PCOS Myths: What You Really Need to Know
Common Questions About PMOS
Q: What does PMOS stand for?
A: PMOS stands for Polyendocrine Metabolic Ovarian Syndrome. It is the updated name proposed for the condition previously known as Polycystic Ovarian Syndrome (PCOS).
Q: Is PMOS the same as PCOS?
A: Yes, PMOS and PCOS refer to the same underlying condition. The name has been updated to more accurately reflect the hormonal, metabolic, and systemic nature of the syndrome.
Q: Why was PCOS renamed to PMOS?
A: The term “polycystic” was medically misleading — many women with the condition do not have visible cysts, while many without the condition do. The new name, PMOS, better reflects the endocrine and metabolic nature of the disorder.
Q: Do I need a new diagnosis if I already have PCOS?
A: No. Your existing diagnosis is valid and carries over. You do not need to repeat diagnostic testing simply because the name has changed.
Q: What are the main PMOS symptoms?
A: Irregular periods, excess androgen effects (acne, unwanted hair, hair thinning), weight gain, insulin resistance, fertility challenges, and mood changes are the most common symptoms.
Q: Can PMOS be cured?
A: PMOS cannot currently be “cured” in the traditional sense, but it is highly manageable. With appropriate lifestyle changes, medication, and monitoring, most women live comfortably and healthily with the condition.
Q: Does PMOS affect fertility?
A: It can, primarily through irregular or absent ovulation. However, with proper fertility treatment, the majority of women with PMOS can conceive successfully.
Q: What is the best diet for PMOS?
A: A low-glycaemic, anti-inflammatory diet, rich in vegetables, lean protein, whole grains, and healthy fats, with limited refined carbohydrates and sugar, is most consistently supported by evidence.
Q: Is PMOS treatment different from PCOS treatment?
A: Not currently. The same medications, lifestyle interventions, and fertility treatments apply. Future guidelines may place greater emphasis on metabolic health management.
Q: Should I see a specialist for PMOS?
A: Yes. A gynaecologist, reproductive endocrinologist, or fertility specialist with experience in PMOS/PCOS is best placed to guide your care, particularly if you are trying to conceive.
Takeaway
Here is what we want you to take away from this article:
PMOS is not a new disease. It is a renamed and better understood one. If you have been living with a PCOS diagnosis, everything you have learned about managing your condition, the dietary changes, the medications, the fertility treatments, the monitoring, remains valid, useful, and effective.
The shift from PCOS to PMOS is medicine doing what it is supposed to do: refining its language to more honestly reflect reality. And in doing so, it opens the door to better, more comprehensive care. One that treats not just your ovaries, but your hormones, your metabolism, your mental health, and your whole life.
You are not starting over. You are building on a foundation that was already there.
If you have questions about your PMOS diagnosis, are trying to conceive, or simply want a clear-eyed conversation with a specialist who understands this condition deeply, Ferty9 Fertility Center is here for you.
Early diagnosis, personalised care, and the right support make an enormous difference. You deserve all three.
Ferty9 Fertility Center – Compassionate Care. Evidence-Based Practice. Real Results.
















 No need to worry, your data is 100% safe with us!
No need to worry, your data is 100% safe with us!