
Myth 1: Irregular periods are a definitive sign that you have PCOS
The Fact: While irregular periods are a prevalent symptom of PCOS, they are not the only cause of an irregular menstrual cycle. Many other factors can throw your cycle off track.
A. Understanding Irregular Periods
First, what exactly are irregular periods? A “normal” menstrual cycle is around 28 days, but it can vary from 21 to 35 days. Periods are considered irregular if:
- The time between periods varies significantly each month.
- You miss periods altogether (amenorrhea).
- You have periods more frequently than every 21 days or less frequently than every 35 days.
- The length or heaviness of your flow changes drastically.
B. What is PCOS?
PCOS is a hormonal disorder characterized by a combination of at least two of the following:
- Irregular Ovulation: Leading to irregular, infrequent, or absent periods.
- High Levels of Androgens: These “male” hormones can cause symptoms like excess facial and body hair (hirsutism), acne, and male-pattern baldness.
- Polycystic Ovaries: On an ultrasound, the ovaries may appear enlarged and contain numerous small follicles (immature eggs). However, it’s important to note that not all women with PCOS have visible cysts on their ovaries.
C. The Link Between Irregular Periods and PCOS
In PCOS, hormonal imbalances, particularly high androgens (male hormones) and issues with insulin regulation, often disrupt the normal ovulation process. This lack of regular ovulation is a primary reason why women with PCOS experience irregular periods.
Irregular periods are a key symptom of Polycystic Ovary Syndrome (PCOS), but they don’t necessarily indicate the condition. It’s essential to consult a doctor for a diagnosis, who can evaluate symptoms and medical history, and perform tests like blood tests and ultrasounds. It’s crucial to avoid common myths and seek professional medical advice. The image of an ultrasound screen, often associated with PCOS, may be misleading, as it may not accurately diagnose the condition. It’s essential to separate the myth from the fact and understand the nuances of your body.
While PCOS makes cycles unpredictable, logging your dates in an accurate Period Calculator helps identify the subtle patterns in your unique hormonal rhythm.
Myth 2: A pelvic ultrasound is enough to declare a diagnosis of PCOS
The Fact: While an ultrasound is a valuable tool in diagnosing PCOS, it is not the sole determinant. A diagnosis of PCOS relies on a combination of factors, and a scan alone is insufficient.
A. Understanding the Rotterdam Criteria
The most widely accepted criteria for diagnosing PCOS are the Rotterdam criteria. According to these guidelines, a woman needs to meet at least two out of three of the following criteria for a PCOS diagnosis, after excluding other possible conditions:
- Irregular Ovulation: This leads to irregular, infrequent, or absent periods.
- Clinical and/or Biochemical Signs of Hyperandrogenism: This means either physical signs of high “male” hormones (like excess hair growth, acne, or male-pattern hair loss) or blood tests confirming elevated androgen levels.
- Polycystic Ovaries on Ultrasound: This refers to the appearance of 20 or more follicles (small, fluid-filled sacs) in each ovary, measuring 2-9 mm in diameter, and/or an increased ovarian volume (>10 ml).
B. Why Scanning Alone Isn’t Enough?
Polycystic Ovaries and PCOS
- Polycystic ovaries are common in healthy women without PCOS.
- A significant percentage of reproductive-age women may have them without meeting other criteria.
- PCOS can exist without visible cysts, as some women meet other diagnostic criteria.
- Adolescent ovaries often have multiple follicles, leading to overdiagnosis.
- Ultrasound findings are often interpreted cautiously in adolescents.
- Diagnosis should consider hormonal imbalances, menstrual cycle, and physical appearance.
C. The Diagnostic Process
When a doctor suspects PCOS, they will examine as follows:
- Take a detailed medical history: This includes questions about your menstrual cycles, symptoms of hyperandrogenism, weight changes, and family history.
- Perform a physical exam: They will look for signs of excess androgens like hirsutism and acne.
- Order blood tests: These tests help to measure hormone levels, including androgens, and rule out other conditions.
- May recommend a pelvic ultrasound: This is used to visualize the ovaries and uterus, but is interpreted in conjunction with the other findings.
Myth 3: All women with PCOS are either obese or overweight
The Fact: This is false. PCOS affects women of all shapes and sizes. While insulin resistance, a common feature of PCOS, can contribute to weight gain and difficulty losing weight, it doesn’t affect every woman with the condition in the same way. Many women with PCOS have a healthy weight or are even lean.

A. Understanding the Link Between PCOS and Weight
- Insulin Resistance: A key factor in PCOS for many women is insulin resistance. This means the body’s cells don’t respond effectively to insulin, a hormone that regulates blood sugar. As a result, the pancreas produces more insulin, which can lead to increased androgen production (male hormones) and can also promote fat storage.
- Hormonal Imbalances: The hormonal imbalances characteristic of PCOS, including elevated androgens, can also contribute to weight gain, particularly around the abdomen.
- Metabolic Differences: Some women with PCOS may have differences in their metabolism that make weight management more challenging.
B. Why the Myth is Incorrect
- Many women with PCOS have irregular periods and high “male” hormones, even if they are not overweight.
- Variable degrees of insulin resistance affect weight differently among women with PCOS.
- Genetics and lifestyle factors, like diet and exercise, significantly influence a woman’s weight.
- The Rotterdam criteria for PCOS diagnosis focus on irregular ovulation, hyperandrogenism, and polycystic ovaries on ultrasound, not weight.
C. The Importance of Recognizing Lean PCOS
The misconception that all women with PCOS are overweight can lead to:
- Delayed or Missed Diagnosis: Lean women with PCOS might have their symptoms dismissed or misattributed to other causes because they don’t fit the stereotypical image.
- Feelings of Isolation: Women with lean PCOS might feel like they don’t “belong” in PCOS support groups or discussions.
- Inadequate Management: Healthcare providers might not fully address the hormonal imbalances and other health risks associated with PCOS in lean individuals.
Myth 4: Women with PCOS cannot get pregnant
The Fact: This statement is categorically false. While PCOS is a leading cause of infertility, it does not mean that pregnancy is unattainable for all women with the condition. Many women with PCOS do conceive naturally, and for those who face difficulties, various effective treatments are available to improve their chances of getting pregnant.
A. Understanding How PCOS Can Affect Fertility
The hormonal imbalances characteristic of PCOS often disrupt the regular ovulation process. This can lead to:
- Infrequent Ovulation (Oligoovulation): A Woman may not release an egg every month, making it harder to time intercourse for conception.
- Lack of Ovulation (Anovulation): In some cycles, a woman may not release an egg at all.
These ovulation issues are the primary reason why women with PCOS may experience difficulties getting pregnant.
B. Why the Myth is not correct
- Many Women with PCOS Ovulate Sometimes: Even with irregular cycles, many women with PCOS do ovulate sporadically. If intercourse is timed correctly during these ovulatory windows, natural conception is possible.
- Lifestyle Modifications Can Help: For some women with PCOS, making healthy lifestyle changes, such as losing weight (if overweight or obese), adopting a balanced diet, and engaging in regular exercise, can help regulate their hormones and improve ovulation, increasing the chances of natural conception.
- Effective Fertility Treatments Exist: A range of fertility treatments are available to help women with PCOS conceive. These include:
- Ovulation Induction Medications: Drugs like clomiphene citrate and letrozole stimulate ovulation, aiding egg production and release.
o Gonadotropins: Injectable hormones used under fertility specialist guidance.
o Metformin: Managing insulin resistance, can regulate cycles and improve ovulation in PCOS women.
o Surgical Options: Ovarian drilling may lower androgen levels and improve ovulation, less commonly used due to medical treatments.
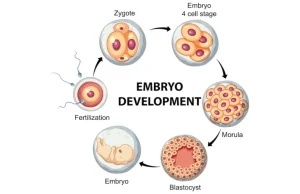
o Assisted Reproductive Technologies (ART): Intrauterine Insemination (IUI) and In Vitro Fertilization (IVF) can improve pregnancy chances. IVF bypasses ovulation by retrieving eggs, fertilizing them, and transferring healthy embryos.
- Success Rates are High: With appropriate diagnosis and treatment, many women with PCOS successfully conceive and have healthy pregnancies. The success rates vary depending on individual factors and the chosen treatment method.
C. The Importance of Seeking Guidance
If you have PCOS and are trying to conceive or planning to in the future, it’s crucial to consult with a healthcare provider or a fertility specialist. They can:
- Assess your situation: Understand your specific PCOS symptoms and ovulation patterns.
- Provide personalized advice: Recommend lifestyle modifications and/or fertility treatments tailored to your needs.
- Monitor your progress: Track your ovulation and receive support from doctors throughout your fertility journey.
PCOS is a common and effective treatment for certain symptoms, but the belief that taking a standard 21-day course of birth control pills can “reduce” or even cure the condition is a significant misunderstanding. It is essential to clarify the facts.
Myth 5: Taking birth control pills can reduce or cure PCOS
The Fact: This is incorrect. While 21-day (or extended cycle) birth control pills are a valuable tool in managing some symptoms of PCOS, they do not reduce or cure the underlying hormonal imbalances and metabolic issues that define the syndrome. They essentially work by masking or regulating certain symptoms while you are taking them.
A. How Birth Control Pills Affect PCOS Symptoms
Combination birth control pills (containing both estrogen and progestin) can be prescribed for women with PCOS to help manage several common symptoms:
- Regulate Menstrual Cycles: Provide monthly withdrawal bleeds for women with irregular or absent periods.
- Reduce Androgen Levels: Help lower the ovaries’ production of androgens.
- Improve Acne and Hirsutism: Lower androgen levels improve acne and hair growth.
- Protect Against Endometrial Hyperplasia and Cancer: Reduce the risk of endometrial hyperplasia and cancer, especially in women with infrequent periods due to PCOS.
B. Why Birth Control Pills Don’t “Reduce” PCOS
- Address Insulin Resistance: Birth control pills focus on hormonal regulation, not directly addressing insulin processing.
- Change Ovarian Morphology: While on the pill, hormonal environment changes can temporarily affect the ovaries.
- Cure Hormonal Imbalance: Pills provide synthetic hormones that override natural cycles, causing underlying hormonal imbalances.
- Do Not Treat Root Cause: Pills provide a consistent hormonal environment, but do not address fundamental issues with hormone production and regulation.
C. The Importance of Comprehensive Management
Effective management of PCOS often involves a multi-faceted approach that may include:
- Lifestyle Modifications: Diet, exercise, and weight management (if applicable) can have a significant impact on insulin resistance and hormonal balance.
- Medications for Specific Symptoms: In addition to birth control pills, other medications like metformin (for insulin resistance), anti-androgens (to directly address high androgen levels), and ovulation induction drugs (for fertility) may be prescribed.
- Regular Monitoring: Ongoing assessment of symptoms and hormone levels is important for long-term management.
Myth 6: If I have regular periods, I don’t have PCOS
The Fact: While irregular periods are a major diagnostic criterion for PCOS, it is possible to have PCOS even with regular menstrual cycles. This is because the diagnostic criteria for PCOS, known as the Rotterdam criteria, require the presence of at least two out of three of the following:
- Irregular Ovulation: Leading to irregular, infrequent, or absent periods.
- Clinical and/or Biochemical Signs of Hyperandrogenism: Physical signs of high “male” hormones (like excess hair growth, acne, male-pattern hair loss) or blood tests confirming elevated androgen levels.
- Polycystic Ovaries on Ultrasound: The appearance of 20 or more follicles on each ovary.
A. Why Regular Periods Don’t Exclude PCOS
- Some women with PCOS may have regular ovulation but still have high androgen levels, causing symptoms like hirsutism or acne.
- Some women may experience milder forms of hormonal imbalances, leading to consistent periods.
- Regular bleeding doesn’t always imply regular ovulation; withdrawal bleeds can occur without consistent egg release.
- Age can influence menstrual cycle regularity, even with other underlying syndrome features.
- Hormonal contraceptives can mask irregularities, causing withdrawal bleeds but not confirming PCOS.
B. What to Look for Beyond Irregular Periods
If you have regular periods but are experiencing other symptoms commonly associated with PCOS, it’s still important to consult your doctor. These symptoms can include:
- Excess hair growth (hirsutism) on the face, chest, or back.
- Persistent acne beyond adolescence.
- Thinning hair or male-pattern baldness.
- Difficulty getting pregnant.
- Weight gain or difficulty losing weight.
- Darkening of the skin in skin folds.
















 No need to worry, your data is 100% safe with us!
No need to worry, your data is 100% safe with us!